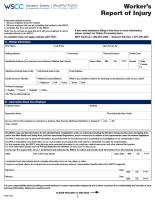
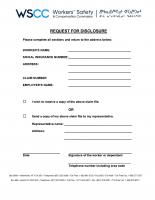
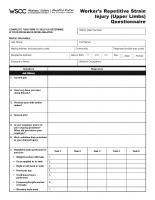
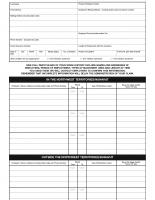
Please read each form carefully to ensure you accurately complete it.
Please contact us at 1-800-661-0792 if you need assistance.
The WSCC collects personal information to administer programs and services related to your claim. For more information please read our Privacy Statement for Workers.